
Contents
- What is cholesterol and what does it do?
- Is cholesterol important for our body?
- What is high blood cholesterol?
- Causes of high cholesterol
- Genetic Factors as a cause of high cholesterol
- Obesity as a cause of high cholesterol
- Stress as a cause of high cholesterol
- Smoking as a cause of high cholesterol
- Lack of exercise as a cause of high cholesterol
- Bad diet as a cause of high cholesterol
- Diabetes Mellitus as a cause of high cholesterol
- Hypothyroidism as a cause of high cholesterol
- Nephrotic syndrome as a cause of high cholesterol
- Anorexia Nervosa as a cause of high cholesterol
- Monoclonal gammopathy as a cause of high cholesterol
- Liver cirrhosis as a cause of high cholesterol
- Primary biliary cirrhosis as a cause of high cholesterol
- Cushing’s syndrome as a cause of high cholesterol
- Age and sex as causes of high cholesterol
- Drugs as a cause of high cholesterol
- High cholesterol treatment
- Lowering cholesterol levels with lifestyle changes
- Drug treatment of high cholesterol
- Complications of high cholesterol
What is cholesterol and what does it do?
Cholesterol is a lipid that is synthesized in the cells in our body. It is one of those essential molecules which are important for life and nearly all cells in the body are capable of synthesizing these lipid molecules. It is can also ingested from animal derived foods.
Cholesterol is a lipid soluble substance that is even though carried through the bloodstream but does not mix in blood because blood is water soluble. For easy transfer of cholesterol through the blood stream, it is packed in combination with protein molecules. These molecules are called as lipoproteins. Lipoproteins are classified into three types:
- Low density lipoproteins (LDL) – called as ‘bad’ cholesterol
- High density lipoproteins (HDL) – called as ‘good’ cholesterol
- Very low density lipoprotein (VLDL)
Is cholesterol important for our body?
Cholesterol is utilized in the body for a variety of purposes. It acts a precursor in the synthesis of Vitamin D in skin. When exposed to sunlight, through a series of reaction, cholesterol is converted to Vitamin D (Cholecalciferol). It is an important component required for proper nerve functions. Nerves are covered with myelin sheath which is made up of cholesterol and fat.
Moreover, adrenal and gonadal hormones are also made up of cholesterol. These hormones are released during stress and are energy handling and reproductive hormones. For the complete and proper development, infant’s brain needs cholesterol.
Human breast milk contains a large amount of cholesterol. Recent studies have revealed that it has been helpful in older patients with declining memory. It also helps in making of the digestive bile acids in the intestines. It also helps in the digestion of food in the gastrointestinal tract.
To perform many of its functions, the route of cholesterol transfer is that it is transported from liver to cells, tissues and glands on low density lipoprotein carriers. The reverse transport is done by high density lipoprotein carriers.
Cholesterol is only found in animal tissues where it is a component of cell membrane. This is the reason why there is more cholesterol in lean tissues rather than in adipose cells.
Cholesterol synthesis is increased to a greater extent from the consumption of polyunsaturated fatty acids than those synthesized from the consumption of saturated fatty acids.
This is primarily because the polyunsaturated fatty acids are deposited in the cell membranes as a result of which body needs to add more cholesterol in these membranes to stabilize them and maintain their fluidity. Cholesterol, when animal derived food is consumed, only about 50% is absorbed.
What is high blood cholesterol?
When the synthesis of cholesterol is more or the utilization of cholesterol in places where it is used is less, the blood cholesterol levels are raised. The increase in blood cholesterol levels can also be due to high intake of saturated fatty acids. The condition itself does not present any signs or symptoms which is a major drawback because many people are unaware that their blood cholesterol levels are high.
It has been recommended that everyone above 20 years of age should get tested for cholesterol every 5 years. This test is commonly known as ‘Lipid Profile’ which is done after 8-10 hours of fasting. This test gives information on
- Total cholesterol levels
- LDL
- HDL
- Triglycerides
For determining the levels of cholesterol on body, a general range is set, which is as follows:
| Total Cholesterol Level | Category |
|---|---|
| Less than 200 mg/dL | Desirable |
| 200-239 mg/dL | Borderline High |
| 240 mg/dL and above | High |
The lipoprotein panel will give your healthcare provider information about your:
-
Total cholesterol. Total cholesterol is a parameter that measures the total amount of cholesterol in your blood, including low-densitylipoprotein (LDL) cholesterol and high-density lipoprotein (HDL) cholesterol.
-
LDL cholesterol. LDL, or “bad,” cholesterol is the main source of cholesterol buildup and blockages in the arteries.
-
HDL cholesterol. HDL, or “good,” cholesterol helps remove cholesterol from systemic circulation.
-
Triglycerides. Triglycerides are also a type of fat found in your blood. Some studies suggest that a high level of triglycerides in the blood may raise the risk of causing coronary heart disease, especially in women.
Causes of high cholesterol
Hypercholesterolemia or high levels of cholesterol in the blood can be caused by a number of factors, some of which are modifiable such as obesity, diet, stress, exercise and some are non-modifiable such as genetic factors.
Apart from there are a number of medical conditions which increase circulating cholesterol levels such as diabetes mellitus type 2, obesity, alcohol, monoclonal gammopathy, dialysis, nephrotic syndrome, hypothyroidism, Cushing’s syndrome, anorexia nervosa.
Finally there are medications which affect cholesterol metabolism and excretion and therefore they may also cause hypercholesterolemia. Usually a person suffering from hypercholesterolemia is at risk due to presence of multiple risk factors.
Genetic Factors as a cause of high cholesterol
A small proportion of all people suffering from hypercholesterolemia have an inherited form of hypercholesterolemia. The most common cause of inherited high cholesterol is due to mutations of the gene LDLR. This condition is known as familial hypercholesterolemia.
The LDLR gene is translated for making a protein called low-density lipoprotein receptor. This type of receptor binds to particles circulating low-density lipoproteins (LDLs), which are the primary carriers of cholesterol in the blood and removes them from the blood.
This way these receptors play a vital role in reducing circulating cholesterol levels. Mutation in this gene will result in either a reduced number of LDL receptors being synthesized or it will disrupt the receptors’ ability to remove low-density lipoproteins from the bloodstream.
Other mutations which cause dyslipidemias particularly hypercholesterolemia are mutations in the APOB, LDLRAP1, or PCSK9 gene. Another form of inherited hypercholesterolemia known as familial defective apolipoprotein B-100 (FDB) is due to mutations of the APOB gene.
Mutations of the LDLRAP1 gene result in another type of inherited high cholesterol called autosomal recessive hypercholesterolemia (ARH). These genes make proteins which are essential for the normal function of low-density lipoprotein receptors; therefore mutations in any of these genes can alter the receptors’ function or prevent the cell from making functional receptors.
Most of these mutations have an autosomal dominant pattern of inheritance while the LDLRAP1 gene has an autosomal recessive pattern. Despite the identification of these genes, it has been found that mutations in a single gene usually do not result in high cholesterol and it is also the presence of environmental factors which triggers the effect of these genes.
Also there is huge variation in the effect of these mutations and these effects vary person to person. Therefore it has been postulated that other genes might also have an impact on the normal function of the LDL receptors and researchers are trying to find out the complete set of genes which is responsible for metabolism of cholesterol.
This way they are hopeful of finding the ‘missing link’ between hypercholesterolemia and genetic factors responsible for it.
Obesity as a cause of high cholesterol
Obesity has been linked with a derangement of the entire cholesterol panel. It has been linked with a decreased amount of HDL (good cholesterol) and increase and increase in triglycerides and LDL (bad cholesterol). Basically the body’s response to the changes in dietary fats is diminished. Following theories have been suggested for this:
- The pathways which synthesize, use and excrete LDL are disturbed so that more LDL is produced than is excreted. Ideally it should be the opposite when large amounts of dietary fats are consumed however there is hormonal disturbance in obesity and the close regulation of LDL levels is lost leading to hypercholesterolemia.
- One of the complications of obesity is inflammation. It has been suggested that the cytokines released during inflammation have a role in blunting the metabolic response to consuming fats.
- Insulin resistance is another common finding in obesity. While the common understanding is that insulin is responsible for storing carbohydrates in the body, however its function is much more than that. This hormone acts as a regulator for a couple of vital steps in the fat metabolism pathways, so when cells become resistant to insulin, insulin no longer reaches the site of metabolism (which is happening inside the cell) and as a result there is a deranged response of body to consuming fats.
Stress as a cause of high cholesterol
The relationship between stress and high cholesterol levels has been studied and while the exact cause is unknown, two well-known and currently accepted reasons for this association are as follows:
- One study concluded that when a person is under stress he is unlikely to care about himself and then develops poor dietary habits and may even put on some extra weight. Both these factors are known to contribute towards high cholesterol. This was found to be particularly true in men.
- When under stress, there is an inflammatory response in our body. To overcome this and to prepare for a potential ‘fight or flight’ situation, the adrenal glands of our body secrete adrenaline as well as cortisol. The short term beneficial effect of these hormones is that they increase the blood flow to the brain and provide an increase amount of energy for our body. The do so by breaking down the stores of glycogen in the liver. In the presence of stress, these hormones will be secreted for longer periods of time and this prolonged hyperglycemia will activate the pathway which converts glucose to triglycerides and eventually cholesterol.
Another theory which stems out from the same concept is that if these hormones stay in the body for longer periods of time, they start to break the fats as well and this will cause the circulating cholesterol levels in our bloods to rise.
Smoking as a cause of high cholesterol
Smoking is another environmental factor which has been associated with high cholesterol levels.
The most well-known effect of smoking on the body is that decreases the levels of the protective cholesterol, HDL. It does so by putting the cholesteryl ester transfer protein (CETP) into overdrive. This protein mediates the transfer of HDL to LDL cholesterol.
So the net effect is that HDL levels are reduced and converted to a form of cholesterol which is difficult to excrete causing hypercholesterolemia. When the HDL levels are decreased, their beneficial effects are lost and the smoker becomes susceptible to heart disease.
Another effect of smoking is that acrolein in cigarettes inhibit the enzyme which keeps the LDL molecule intact. When this enzyme is inhibited the LDL molecule disintegrates and becomes susceptible to oxidation.
After oxidation the molecule structure of LDL is changed and our immune system starts treating the oxidized LDL as a foreign agent releasing white blood cells against it. These cells bring about an inflammatory response which damages the blood vessels, particularly coronary arteries of our heart.
Lack of exercise as a cause of high cholesterol
Regular exercise causes a decrease in LDL levels and increase in HDL levels. Exercise stimulates the transfer of LDL from the blood to the liver from where it is either converted to HDL or excreted into the bile. Therefore a person not doing enough exercise will lose this beneficial affect that exercise brings and will be at high risk of developing hypercholesterolemia.
Severe intensity exercise is more beneficial that moderate intensity, however if you have not being exercising for years now you should consult your doctor first so that he can evaluate for cardiovascular fitness through treadmill test.
Bad diet as a cause of high cholesterol
The two most well-known offenders in our diet which cause an increase in cholesterol levels are saturated fats and trans fats.

Saturated fat and cholesterol are found in foods that originate from animals, such as meats, egg yolks, whole milk, butter, and cheese. It is found to raise total blood cholesterol levels and low-density lipoprotein (LDL) cholesterol levels. They have been linked with an increased risk of developing type 2 diabetes.
Trans fat is mainly found in packaged foods and fried foods, such as chips, cookies, and crackers and have been linked to increase unhealthy LDL cholesterol and lower healthy high-density lipoprotein (HDL) cholesterol.
Diabetes Mellitus as a cause of high cholesterol
Diabetic dyslipidemia is the term given to the lipid profile changes seen in diabetes and is classically characterized by high plasma triglyceride concentration, low HDL cholesterol concentration and increased concentration of small dense LDL-cholesterol particles.
Multiple Risk Factor Intervention Trial (MRFIT) studied the relationship between total cholesterol and cardiovascular disease mortality. It was found that hypercholesterolemia and mortality are directly related. However, if a person is also suffering from diabetes, the spike in mortality is rather dramatic and hence worrisome.
Patients suffering from non-insulin dependent diabetes mellitus or type II diabetes mellitus show increased amounts of free fatty acids in their plasma. These fatty acids are attributed to inhibit insulin-stimulated glucose uptake into muscle and hence cause insulin resistance. Increased amounts of free fatty acids in their plasma would mean that they will now be increased transport of these molecules into the liver.
There they are seen to stimulate a cascade of events which will lead to the production and then secretion of VLDL (major source of triglyceride) into the blood. When VLDL is secreted, its triglyceride is exchange for HDL cholesteryl ester. The resultant HDL molecule is triglyceride rich and becomes a substrate for hepatic lipase or lipoprotein lipase.
When the TG-rich HDL undergoes hydrolysis by these enzymes, the molecular structure is changed and the major HDL protein, apolipoprotein A-I or apoA-I for short can no longer bind with the lipid-poor HDL. As a result HDL molecule disintegrates and apoA-I is then excreted in the urine.
These events are the reason why there is high plasma triglyceride concentration, low HDL cholesterol concentration and increased concentration of small dense LDL-cholesterol particles.
Thus, increased free fatty acid transport in plasma which leads to an insulin-resistant states, may be the underlying cause for the lipid abnormalities seen in diabetes collectively called ‘diabetic dyslipidemia’.
Hypothyroidism as a cause of high cholesterol
Hypothyroidism is another endocrine disease which causes an increase in cholesterol levels. It is now a well-documented fact that thyroid hormones stimulate the 3-hydroxy-3-methylglutaryl-coenzyme A (HMG-CoA) reductase enzyme, which is the first step in cholesterol biosynthesis.
Furthermore, triiodothyronine (T3) binds with its intracellular receptor and then the hormone-receptor complex binds with the specific thyroid hormone responsive elements on the LDL receptor gene to stimulate the production of LDL receptors.
As discussed before, these receptors function to remove the circulating LDL. Therefore hypothyroidism, in which there is decreased plasma thyroid hormone concentration, will lead to hypercholesterolemia.
Another interesting idea is that it is actually the high levels of TSH and not a decrease in thyroid hormones which cause increase in cholesterol levels. In this regard, two authentic studies were carried out in China. The inclusion criteria was that only those patients can become part of this who were not taking any medications nor had health problems that could impact the TSH, thyroid hormone or cholesterol tests.
Both these studies found that there as the TSH levels rise, the blood cholesterol levels rise too. This holds true even when TSH levels are at the upper limit of the normal range and the patient is not suffering from hypothyroidism. Therefore, these studies hypothesize that TSH levels may also effect on the lipid profile and that this is not dependent on the thyroid hormone levels
Nephrotic syndrome as a cause of high cholesterol
Nephrotic syndrome is a set of abnormalities in kidney functions that lead to low serum levels of albumin and caused edema in such patients. In patients suffering from such patients there has been, both increased synthesis and has been a decrease in the clearance of lipoproteinemia. This has often complicated the disease and has led to increased lDL molecules.
This hyperlipoprotenemia may also be linked with increased levels of triglycerides in blood, thus increasing the concentration of Apo C, Apo E and Apo B molecules.
This increase in the synthesis is possibly due to increased availability of mevalonate as a substrate in the synthesis of cholesterol. Moreover, urinary loss of HDL molecules and other major liporegulatory factors causes a decrease in the activity of lipolytic enzymes. All this has led to the impairment in clearance cholesterol and triglyceride thus leading to high blood levels.
Anorexia Nervosa as a cause of high cholesterol
Anorexia nervosa is an eating disorder leading to disturbance in a person’s body weight and eventually changes in shape. There have been cases where the patients have suffered from dangerous levels in decrease in body weight. However, it has been observed in such patients that these patients have surprisingly high plasma levels of cholesterol in their bodies.
People suffering from anorexia nervosa are basically avoiding the intake of food with calories and since these food also contain enough amounts of cholesterol that can contribute significantly to increase in weight. However, there has been an unusual trend. The high cholesterol levels of cholesterol in these patients are possibly due to genetic mutation.
Over 150 genes are linked either directly or indirectly with this disorder. Research has shown that mutation in any one of these genes especially that which is linked which is responsible with the production of cholesterol both due to dietary intake and internal cholesterol.
This genetic mutation has also largely contributed towards behavioral changes. In anorexic patients, the assumptions are made that their abilities to withstand severe malnutrition is made easier for the patients to survive.
Monoclonal gammopathy as a cause of high cholesterol
Patient suffering from monoclonal gammopathy have been observed with low HDL phenotype and there have been accumulation of cholesterol molecules. This accumulation of cholesterol was due to the reduction of HDL capacity of promoting cholesterol efflux from macrophages.
When high levels of plasma cytokines (TNFα and IL-6), soluble cytokine receptors were observed in patients suffering from necrobiotic xanthogranuloma with monoclonal gammopathy. This revealed a specific xanthoma which correlated with the plasma levels of anti-inflammatory HDL. These xanthomas are yellowish cholesterol rich material present in large sized foam cells.
Studies have recently proved that necrobiotic xanthogranuloma is described by impaired lipid macrophage homeostasis associated with a systemic inflammatory profile. This inflammatory may be a result from possible interaction of Mlg (monoclonal immuglobulin) and lipoproteins.
Pathalogically this has caused the formation of lesions on skin or in visceral regions which are due to cholesterol accumulation and monoclonal immunoglobulin (MIg). The lesions were mostly nodules or plaques. Monoclonal gamopathy therapy can be thus a very useful treatment.
Liver cirrhosis as a cause of high cholesterol
Liver is the center of metabolism for all pathways; hence it is not surprising that when it is suffering from disease, particularly liver cirrhosis, all its metabolic functions will be disrupted. As a result breakdown of triglycerides and LDL will be reduced leading to both hypercholesterolemia and hypertriglyceremia.
Other possible mechanisms suggested for this decrease are increased supply in diet (people consuming medicine from non-authentic practitioners are found to have a number of adulterations and since their liver is not functionally correctly, there might be accumulation of those adulterations and nutrients).
A rather unusual finding in some of these patients is that while their lipid profile is disturbed, they show no increase incidence of cardiovascular events. One of the reasons is that a diseased liver goes into protective mode and secretes more HDL, which is cardio protective.
However other studies have found that while in some cases HDL may rise; people suffering from nutritional deficiency or familial hypercholesterolemia still show a lower HDL level so there must be another reason for this.
Primary biliary cirrhosis as a cause of high cholesterol
Primary biliary cirrhosis is an autoimmune disease of hepatobiliary tract characterized by slow, progressive destruction of the small bile ducts of the liver, causing bile and other toxins to build up in the liver, a condition called cholestasis.
Cholesterol is an important constituent of bile, a fluid produced by liver and stored in the gallbladder which aids in the digestion of fats. Destruction of passages, first extrahepatic and then intrahepatic, and then the acini (secretory cells arranged in glandular form are called acini) will setup a situation where cholesterol is no longer utilized for this purposes leading to its accumulation and casing hypercholesterolemia.
Cushing’s syndrome as a cause of high cholesterol
Cushing’s syndrome is a collection of symptoms and signs shown by the body due to prolonged exposure to cortisol. Cortisol, a glucocorticoid, causes hyperglycemia and prolonged hyperglycemia will activate the pathways which convert blood sugar into lipids including cholesterol.
Age and sex as causes of high cholesterol
Starting at puberty, men often have lower levels of HDL cholesterol compared to women. As women and men age, their LDL cholesterol levels in blood often rise. Before age 55, women usually have lower LDL cholesterol levels than men. However, after age 55, women can have higher LDL levels than men.
Drugs as a cause of high cholesterol
There are a number of drugs which can cause hypercholesterolemia. The pathophysiology is different for each drug.
- Diuretics: Both thiazide diuretics (hydrochlorothiazide, metalozone) and loop diuretics (furosemide) can cause hypercholesterolemia. The mechanism is unknown but it is thought to be due to worsened insulin sensitivity and/or reflex activation of the renin-angiotensin-aldosterone system (RAAS) and sympathetic nervous system in response to volume depletion.
- Amiodarone: This drug decreases plasma and tissue triiodothyronine (T3) due to which there is hypercholesterolemia
- Beta blockers: β receptors are present on a number of tissues including pancreas and skeletal muscle. So when β blockers without intrinsic sympathetic activity block these receptors, there is a slight metabolic disturbance in some people causing hypercholesterolemia.
- Steroids: They cause hypercholesterolemia the same way steroidal hormones cause in stress or Cushing’s syndrome.
- Anticonvulsants: Phenytoin and carbamazepine are two anticonvulsants notorious for causing raised cholesterol levels. They do so by stimulation of hepatic enzymes, one of which is cholesterase. They also increase the hepatic synthesis of bile acids. These acids increase the amount of cholesterol which is being absorbed in the intestines by facilitating micelle formation.
- Birth pills: Birth pills contain estrogen and progesterone. Progesterone decreases HDL and increases LDL while estrogen does the opposite. Therefore it is recommended that birth pills should contain more estrogen than progesterone but even after this one should take these pills with caution.
- Others: cyclosporine and protease inhibitors are other drugs which cause high cholesterol however the mechanism by which they do so is still unknown.
High cholesterol treatment
The main focus in cholesterol lowering treatment is to decrease the levels of low density lipoproteins (LDL) – the bad cholesterol. The higher the number of LDL molecules, the greater the risk for the person to develop heart diseases. There are two main ways to lower the cholesterol levels
- Therapeutic lifestyle Changes – this includes a diet consists of food have low cholesterol levels, more physical activity, and proper weight management. This strategy of lifestyle changes is the first and on top most priority for those people who have LDL greater than normal range.
- Drug treatment – when the total cholesterol levels or LDL levels are high in category, drugs either single or in combination of more than one are prescribed along with the recommended changes in lifestyle.
Treatment is made depending on which category is the patient falls into:
- Category I, highest risk: when the LDL is less than 100 mg/dl. The plan is to initiate the low cholesterol diet. This will slow down the process of development of atherosclerotic plaque. If the LDL is 100 or above, it is better to start the drug treatment along with modifications made in lifestyle. However in certain cases here the LDL levels are below 100mg/dl but the patient have recently recovered from heart attack or angina then the doctor will recommend drugs too.
- Category II, Next highest risk: when the LDL levels are 130mg/dl or above, a plan of drug treatment along with lifestyle changes. If the person is only going for lifestyle changes and the goal of 130mg/dl is not achieved even after 3 months, drug treatment is necessary along with lifestyle changes. When the LDL goals are achieved of reaching 130mg/dl, a need for continuing with the healthy diet, which involves a little more intake of saturated fat and cholesterol than with the lifestyle changes.
- Category III, Moderate risk: goal is to keep the LDL levels below 130mg/dl. If the LDL levels after testing is 160mg/dl or above even after 3 months of continuous changes of lifestyles, drug treatment should be started in conjunction to lifestyle changes. When the levels of low density lipoproteins (LDL) decrease below 130mg/dl, all those who are at a risk with heart diseases should maintain their healthy diet.
- Category IV, low to moderate risk: when LDL goals is less than 160mg/dl. If the LDL is 160mg/dl or above, there is a need to start with the recommended lifestyle. However it is preferred to start the drug treatment with physical activities and healthy diet chosen for such a patient, especially when the LDL levels is 190mg/dl or more.
Lowering cholesterol levels with lifestyle changes
Any changes made in ones’ lifestyle for a therapeutic purpose, these are termed as therapeutic lifestyle changes (TLC). TLC include a range of things that can be done to lower the body’s cholesterol levels specifically LDL levels. These include:
- The TLC diet: for patients with high cholesterol levels a change is diet is required. A saturated fat, low cholesterol plan that only provides less than 7 percent of calories from saturated fat and less than 200mg of dietary cholesterol per day. A proper TLC diet demands to maintain a desirable weight and avoid getting overweighed or obese. If the LDL levels doesnot come to a desirable level only by reducing the intake of saturated or high cholesterol containing foods, an alternate that can be implied is to increase the intake of fiber content in diet. Fiber is rich in peas, beans, lentils etc. Another option to make the diet low cholesterol is to utilize those foods containing plant sterols (a well-known example is margarine) with the aim to lower the LDL levels in body. Protein rich food such as legumes which are full of nutritional riches. Nuts and seeds have shown to lower the LDL levels in blood. However to avoid getting overweighed, one must not consume more than 1 ounce daily.
- Weight management: when targeting for lowering blood cholesterol levels, taking a maintained diet is not only what it counts, it also depends on how much the person eats. Losing weight is a helpful strategy to lower the risk of heart diseases. Being overweight increases the chances of having a high level of LDL in blood. This is especially recommended to those who have high triglyceride levels or low HDL. Doctors recommend this to those men who have a waist measurement of more than 40 inches and women with more than 35 inches. However other measures can be taken to reduce the weight.
- While purchasing of food products, one must read the label attached and those giving less calories per serving should be preferred.
- Having 5-6 meals per day is healthier rather than consuming 3 large meals.
- Sodas, soft drinks and alcohol should be avoided.
- Physical activity: a person should on daily basis whether he/she has high cholesterol levels or not, do exercise for at least 30minutes. It not only decreases the body mass but also helps to raise the HDL and lower LDL levels.
Drug treatment of high cholesterol
Medicine is not the first solution to every therapeutic problem. However, when it is necessary the dose of the medicine should be kept as low as possible. However anti-lipids include a variety of drugs. Anti-lipids include statins, bile acid sequestrants, nicotinic acid, cholesterol absorption inhibitors and fibric acids.
Depending on the individual cases, a doctor is at the best position to prescribe which drug is best. The statins are most commonly prescribed. They help to lower LDL but the only drawback is that it can cause myopathy.
Bile acid sequestrants can be used alone or in combination with statins. Fibric acid are preferentially given to lower the triglycerides in blood and raise HDL. Cholesterol absorption inhibitors are given to those who have a habit of eating more.
The first priority when drug treatment is prescribed is to lower the LDL levels. Once it is resolved, then the levels of triglycerides and HDL are considered.
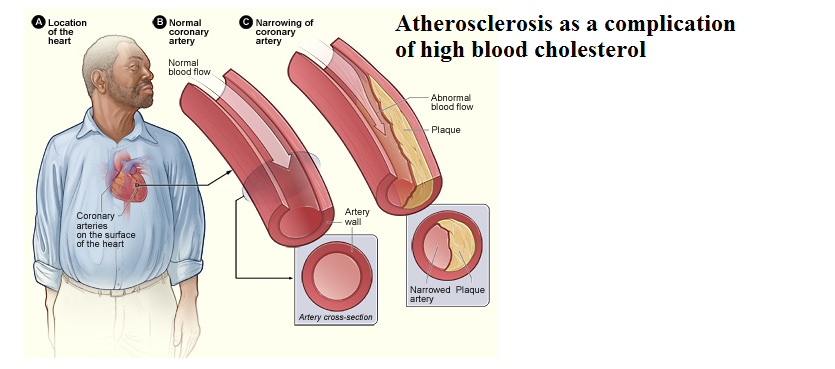
Complications of high cholesterol
The blood cholesterol levels have a lot to cause heart diseases. It is counted as a risk factor. Risk factor is anything that makes a person prone to get a disease. When cholesterol level is higher, it starts accumulating in the arterial walls.
This accumulation leads to the hardening of the walls ultimately constricting the lumen of the artery and decreasing the blood flow. The area where the LDL molecules have accumulated is called as plaque.
When accumulated in the coronary artery has the highest chances to cause heart attack. If the flow of oxygen rich blood to heart is reduced or blocked, angina or heart attack can occur.
Angina is a chest pain or discomfort. It may feel like pressure or squeezing in your chest. The pain may also occur in your shoulders, arms, neck, jaw or back. The pain of angina may be mis understood as indigestion. Heart attack occurs when the blood flow is completely cut off. If not quickly restored, the muscle starves and dies. This can prove fatal also.
However, accumulation can also occur in other arteries that are responsible for providing oxygen rich blood to upper and lower limbs as well as to brain. This in turn will lead to other problems such a peripheral artery disease, stroke etc.
Peripheral artery disease (PAD) occurs when there is buildup of the plaque in the arterial walls those which are supplying blood to kidneys, arms, stomach, legs and feet. With time as PAD progresses, symptoms start to occur more often even when the patient is at rest. People suffering from PAD are more prone to have stroke, heart attack or even limb amputations.
Stroke occurs when the blood flow is reduced or cut off due to blockage by plaque in arterial walls. It is a medical emergency which should be immediately treated. Otherwise the part of brain which that specific nerve is supplying the blood will be deprived and the particular function performed that specific part of the brain is affected. Effects such paralysis, slurring of speech occur.
“How far in advance should you start taking prenatal vitamins with minerals?”
“Does coconut oil lower cholesterol?“